46 gene sequencing test for cancer patients on the NHS
The first multi-gene DNA sequencing test that can help predict cancer patients' responses to treatment has been launched in the National Health Service (NHS), thanks to a partnership between scientists at the University of Oxford and Oxford University Hospitals NHS Trust.
The test uses the latest DNA sequencing techniques to detect mutations across 46 genes that may be driving cancer growth in patients with solid tumours. The presence of a mutation in a gene can potentially determine which treatment a patient should receive.
The researchers say the number of genes tested marks a step change in introducing next-generation DNA sequencing technology into the NHS, and heralds the arrival of genomic medicine with whole genome sequencing of patients just around the corner.
The many-gene sequencing test has been launched through the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC), a collaboration between Oxford University Hospitals NHS Trust and Oxford University to accelerate healthcare innovation, and which has part-funded this initiative.
The BRC Molecular Diagnostics Centre carries out the test. The lab, based at Oxford University Hospitals, covers all cancer patients in the Thames Valley area. But the scientists are looking to scale this up into a truly national NHS service through the course of this year.
The new £300 test could save significantly more in drug costs by getting patients on to the right treatments straightaway, reducing harm from side effects as well as the time lost before arriving at an effective treatment.
'We are the first to introduce a multi-gene diagnostic test for tumour profiling on the NHS using the latest DNA sequencing technology,' says Dr Jenny Taylor of the Wellcome Trust Centre for Human Genetics at Oxford University, who is programme director for Genomic Medicine at the NIHR Oxford BRC and was involved in the work. 'It's a significant step change in the way we do things. This new 46 gene test moves us away from conventional methods for sequencing of single genes, and marks a huge step towards more comprehensive genome sequencing in both infrastructure and in handling the data produced.'
Dr Anna Schuh, who heads the BRC Molecular Diagnostics Centre and is a consultant haematologist at Oxford University Hospitals, adds: 'Patients like the idea of a test that can predict and say up front whether they will respond to an otherwise toxic treatment. What the patient sees is no different from present. A biopsy is taken from the patient's tumour for genetic testing with a consultant talking through the results a few days later. It is part of the normal diagnostic process.'
Cancer is often described as a genetic disease, since the transition a cell goes through in becoming cancerous tends to be driven by changes to the cell's DNA. And increasingly, new cancer drugs depend on knowing whether a mutation in a single gene is present in a patient's cancer cells.
For example, a lung cancer patient may have a biopsy taken to check for changes in the EGFR gene. If there is a mutation, the patient may then be treated with a drug that works as an EGFR inhibitor. If there is no mutation, such drugs won't work and the patient would get a different drug that would be more effective for them. Knowing the presence or absence of mutations in a certain gene can choose the treatment path for that patient.
The NHS can currently test for mutations in 2 or 3 genes – genes called BRAF, EGFR or KRAS – using older sequencing technology that has been around for decades. Efforts are being made to look at increasing the number of cancer genes sequenced to nine as standard.
The Oxford scientists are the first to make such multi-gene tests possible in the NHS using the latest DNA sequencing techniques. The NHS service they have launched looks for mutations in 46 genes, and they are now working towards verifying the use of a test involving 150 genes.
Having a diagnostic test or 'panel' that can screen for mutations in multiple genes at once will be important for access to all the new cancer drugs that are coming along.
'It will be very difficult to manage in NHS diagnostic labs without gene panels,' explains Dr Schuh. 'Currently, new cancer drugs tend to get approved alongside a diagnostic test specific to that drug which can determine which patients will benefit. But as more and more drugs like this come along, we can't possibly run all the many different separate tests this could mean. We need one test for a range of drugs.'
Dr Taylor adds: 'We wanted a test that would use the latest DNA sequencing techniques to detect a wide range of mutations in a wide range of genes. A test that would be able to cover more cancers and more treatments, all for a similar cost to conventional methods.'
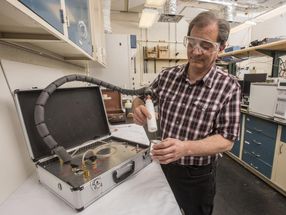
The test is run on a next generation sequencing platform from Life Technologies Corporation, called the Ion Personal Genome Machine (PGM(TM)). The test and accompanying software have been substantially modified as requested by the Oxford team to fulfil diagnostic standards in their lab.
As part of the test development, the Oxford team looked to improve the initial sample preparation in the lab, and to provide the software and infrastructure support to handle and analyse the amount of information involved. Most importantly, the Oxford group has carried out tests and comparisons to verify the robustness of the technique with cancer biopsies direct from patients.
The team compared the new 46 gene test against conventional techniques for 80 consecutive cancer biopsies in the hospital lab's workflow.
The next-generation DNA sequencing method detected all the mutations the conventional method did; it detected new mutations the conventional method didn't; and detected mutations present at much lower levels in the samples. The time taken for the 46 gene test also fitted into the standard turnaround time for samples at the lab.
There is definite benefit in screening some of the 46 genes included in the test; there is probable or likely clinical benefit in screening some of the others; mutations in further genes might be important in some cancers but not others; and the other genes, we don't know as yet. But having this information means researchers can investigate whether a mutation has biological significance.
'We can keep data, bank it and link it with anonymised clinical data on patients' cancers for future research,' explains Dr Schuh.
The test looks for mutations in 'hotspot' regions of each gene – areas where mutations are more likely to occur. This does mean the test may miss up to 5% of mutations, as they can occur elsewhere, but this is still significantly better than the 'false negative' rate using current methods.
It can also detect mutations present in only 5% of the tumour cells present in a sample. This is much lower than is possible currently, and is important in being able to capture information from cells present in only small numbers in a tumour, but which are still important in driving cancer growth.
Having shown that it is possible to introduce the 46 gene test as an NHS service, the researchers are now moving on to investigate the potential of a test that will sequence 150 genes. The team will use the test first of all with 500 existing samples from patients taking part in cancer clinical trials to be able to compare the results retrospectively with information from the trials. They will then use the test with 1000 new cancer biopsies to better understand how the extra information could be used in guiding treatments for patients and their outcomes.
Dr Schuh says: '"Panel" tests have significant potential while we wait for the cost of sequencing whole patient genomes to come down. Even then, panel tests may be with us for some time. After whole genome sequencing does come into use, it may be that panel tests are used first with patients' biopsies, with only those whose panel test shows no result having their entire DNA sequenced to look for rarer genetic changes.'
Lord Howe, Health Minister, said: 'We want to be among the best countries in the world at treating cancer and know that better tailored care for patients could potentially save lives.
'Health research like this is incredibly important and I'm delighted we could support the work of researchers in Oxford through the National Institute for Health Research Biomedical Research Centre.
'By rapidly translating findings from genetics research into real benefits for patients, their work will make sure that patients get the right treatments straight away, reduce potential side effects and also help us use NHS funds more effectively.'
The 46-gene panel is based on Ion AmpliSeq(TM) chemistry from Life Technologies Corporation. The test requires a very small amount of DNA (5 nanograms), an advantage when working with clinical samples that are typically limited in quantity.
The Ion Personal Genome Machine (PGM(TM) and Ion AmpliSeq(TM) are for Research Use Only, not intended for use in diagnostic procedures. Life Technologies intends to pursue CE-IVD designation for the PGM.

Other news from the department science





















Get the life science industry in your inbox
From now on, don't miss a thing: Our newsletter for biotechnology, pharma and life sciences brings you up to date every Tuesday and Thursday. The latest industry news, product highlights and innovations - compact and easy to understand in your inbox. Researched by us so you don't have to.