MEK Inhibitors: A New Weapon in the Fight Against Melanoma
cancer cell signaling has long been an attractive target for oncology drug development. Increased activation of cell survival signaling cascades promotes tumor cell growth and makes cancer cells difficult to kill. Inhibiting proteins that are involved in these survival pathways is one strategy to selectively destroy cancerous cells. The mitogen activated protein kinase (MAPK) pathway is one such signaling cascade that, when activated, promotes cell survival. Preclinical research has found that this pathway is activated in most melanomas; consequently, one of the key kinases involved in this pathway, MEK, has become the focus of targeted therapies for the treatment of melanoma. MEK, which stands for MAPK/ERK kinase and is also known as MAPKK, has several known structural variants called “isoforms” which play different roles within the cell. Isoforms 1 and 2, referred to as MEK1/2, are the isoforms associated with MEK’s ability to promote cell survival.
Another example of oncogenic perturbations to cellular signaling cascades is the hyperactivation of BRAF kinase. Genetic mutations in the BRAF gene encoding this protein are found in 60% of melanomas, and cause the product BRAF protein to be unusually active. Roche/Genentech and Plexxikon, now part of Daiichi Sankyo, have already successfully developed and commercialized Zelboraf (vemurafenib) as a targeted therapy for metastastic melanoma with the V600E BRAF mutation. While BRAF currently may be the more hotly pursued target for melanoma treatments, savvy pharmaceutical companies recognize the potential benefits of attacking multiple signaling pathways at once. Preclinical data has shown inhibition of BRAF frequently has the undesirable effect of further activating MEK-MAPK signaling; it therefore stands to reason that by shutting down this pathway, MEK inhibitors (MEKi’s) may be able to combat resistance to BRAF inhibitors.
At the 2012 ASCO annual meeting, data was presented from GlaxoSmithKline’s (GSK) Phase I/II clinical trial evaluating a combination of its BRAF inhibitor (BRAFi) dabrafenib (GSK2118436) and its oral MEK1/2 inhibitor trametinib (GSK1120212) for the treatment of V600 BRAF mutant solid tumors. Of the 77 BRAFi-naïve melanoma patients enrolled in the trial, the dabrafenib/trametinib combination therapy evoked a confirmed overall response rate of 56%. Of particular interest was the safety profile of this combination; patients taking the dual therapy had a lower incidence of MEKi-related rash and BRAFi-induced hyperproliferative skin lesions compared to patients in trials taking single-agent trametinib or dabrafenib. This data supports the hypothesis that the two drugs are targeting different pathways within the cell, and suggests that some of the adverse events associated with BRAFi monotherapy may be mediated by MEK signaling (and vice versa).
However some very serious adverse events occurred, including squamous cell carcinoma in two patients and actinic keratosis in two patients. These effects are comparable to those occurring with Zelboraf treatment, so they may not significantly obstruct future regulatory approval. The efficacy data from this early stage trial is limited but promising. The overall progression free survival of patients taking any of the dose combinations of trametinib and dabrafenib was 7.4 months, although the trial had no control arm for use as a comparison. GSK is currently sponsoring Phase III clinical trials comparing dabrafenib and trametinib combination therapy to dabrafenib monotherapy or Zelboraf monotherapy for the treatment of unresectable or metastatic BRAF V600E/K positive melanoma. Meeting the primary endpoint of overall survival in the head-to-head trial with Zelboraf would be definitive proof of the clinical benefit of dual BRAF/MEK inhibition.
It is important to note that trametinib is also in development as a monotherapy. Data was presented at ASCO 2012 from a Phase III clinical trial showing trametinib monotherapy demonstrated better efficacy than dacarbazine or paclitaxel monotherapy for treating metastatic BRAF V600E/K positive melanoma. BRAFi- and MEKi-naïve patients treated with trametinib had a median progression free survival of 4.8 months compared to 1.4 months observed in patients treated with dacarbazine or paclitaxel. Current trends suggest an overall survival benefit as well, although the data is not yet mature. While this data is also promising, GlobalData believes that the greatest efficacy benefits of trametinib and other MEK inhibitors will stem from their use in combination therapies.
Roche/Genentech is also aware of the potential efficacy benefits of combined BRAF/MEK inhibition for the treatment of melanoma. Under an agreement with Plexxikon, the companies have already developed and commercialized Zelboraf for the treatment of metastatic melanoma with the V600E BRAF mutation. Not to be outdone by GSK, the companies are now developing their own MEK1/2 inhibitor, GDC‑0973. Roche is currently sponsoring a Phase I clinical trial investigating the safety and pharmacokinetics of Zelboraf in combination with GDC-0973 in metastatic melanoma patients whose cancer has progressed following initial Zelboraf treatment. Unfortunately for Roche, its combination therapy lags far behind GSK’s trametinib which is already in Phase III development.
Combination therapies inhibiting MEK and non-BRAF cellular signaling targets are also in development. At ASCO 2012, data was presented from a Phase Ib trial evaluating the combination of Genentech’s MEK1/2 inhibitor GDC‑0973 and their class I PI3K inhibitor GDC-0941 for the treatment of advanced solid tumors, including melanoma. Dual inhibition of these two pathways is an appealing strategy as constitutive activation of the PI3K-AKT pathway promotes cancer cell survival and is a characteristic of a broad spectrum of cancers. Genentech is investigating inhibition of these two pathways using an alternate combination of GDC-0973 and GDC-0068. GDC-0068 also targets the PI3K-AKT pathway, but at a different point; it inhibits AKT, a kinase involved in the PI3K-AKT signaling cascade, rather than PI3K. However no data from this trial has been presented.
The GDC-0973 and GDC-0941 combination therapy is in the early stages of development, so limited efficacy data is available. However there are very early signs of tumor response, as 26 of 46 evaluable patients had an FTG-PET partial metabolic response at one or more time points. A major concern with combination therapies is whether targeting multiple pathways will compound the side effects associated with each drug; however the toxicities observed with GDC‑0973 and GDC-0941 combination therapy were comparable to those observed with monotherapy treatment.
The use of MEK inhibitors in various combination therapies and as monotherapy is a strategy with strong preclinical roots and growing clinical evidence to support its implementation. GSK will almost certainly be the first company to seek regulatory approval for a MEK inhibitor for the treatment of metastatic melanoma, as trametinib is the most advanced MEK inhibitor in development for this indication. While the data presented at ASCO 2012 is promising, trametinib’s regulatory approval will ultimately depend on positive Phase III results demonstrating the drug increases patient overall survival, especially considering the potential for serious side effects. Combination therapies designed to synergistically target multiple signaling pathways like trametinib and dabrafenib hold great promise for the treatment of cancer due to abundant evidence showing that suppression of a single cascade results in increased signaling through related survival pathways. These treatments are not without their pitfalls, as correct dosing and safety profiles can be major issues. GlobalData believes that these issues can be resolved using intelligently designed clinical trials, and that in the future, targeted combination therapies have the potential to greatly advance the treatment of melanoma and other solid tumors.
These are the results of the report "MEK Inhibitors: A New Weapon in the Fight Against Melanoma" by GlobalData.
Other news from the department business & finance





















Most read news












More news from our other portals






















Last viewed contents
MedImmune to Acquire Cellective Therapeutics, Inc.
Johnson & Johnson announces completion of Novira Therapeutics, Inc. acquisition
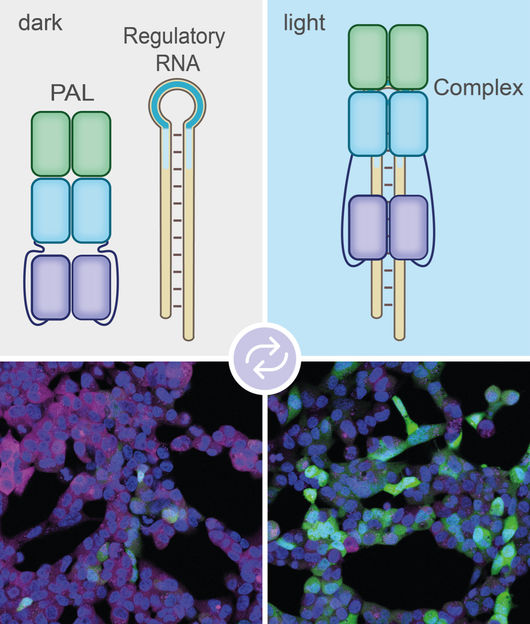
New method allows precise gene control by light - Study enhances research toolbox with a new tool with great potential
New Biomedical Sciences Executive Committee Established to Lead Phase 2 of Singapore's Biomedical Sciences Initiative
